

Snapshot
- A 52-year-old man with a past medical history of diabetes mellitus presents with fever and acute onset left lower quadrant abdominal pain. CT scan with contrast shows acute diverticulitis. He is started on broad-spectrum antibiotics. The next day, daily labs reveal a rise in creatinine from 0.7 mg/dL to 2.0 mg/dL. Urinalysis is obtained and a significant amount of muddy brown casts is found. He is immediately started on intravenous normal saline.
Introduction
- Clinical definition
- intrinsic acute kidney injury (AKI) to the kidneys from ischemia and/or toxins
- Epidemiology
- incidence
- US incidence
- most common cause of AKI in hospitalized patients
- US incidence
- risk factors
- pre-existing kidney disease
- incidence
- Etiology
- nephrotoxic injury
- drugs
- aminoglycosides
- contrast for imaging
- heavy metals
- crystals
- calcium oxalate crystals from ethylene glycol
- urate crystals from tumor lysis syndrome
- myoglobinuria
- hemoglobinuria
- drugs
- nephrotoxic injury
- Pathogenesis
- decreased renal blood flow results in ischemia
- this results in death of renal tubular cells
- in particular the proximal convoluted tubule and thick ascending limb are affected
- nephrotoxicity leads to damage in renal tubules
- in particular proximal convoluted tubule is affected
- decreased renal blood flow results in ischemia
- Prognosis
- 3 stages of disease
- inciting event
- oliguric (maintenance) phase
- 1-3 week duration
- risk of electrolyte abnormalities
- hyperkalemia
- metabolic acidosis
- uremia
- prognostic variable
- negative
- requiring dialysis
- negative
- survival with treatment
- over half of patients fully recover
- 5-11% require long-term dialysis
- 50% mortality in those needing dialysis
- 3 stages of disease
| Classification of Acute Renal Failures | |||
| Urinary Indices | Pre-Renal | Intrinsic Renal | Post-Renal |
| Urine osmolality (mOsm/kg) | > 500 | < 350 | < 350 |
| Urine Na (mEq/L) | < 20 | > 40 | > 40 |
| Serum BUN:creatinine | > 20 | < 15 | < 15 |
| FENa (%) (fractional excretion of Na) | < 1% | > 2% | > 2% |
| FEUrea (%) (fractional excretion of urea) | < 35% | 50-65 % |
Presentation
- Symptoms
- primary symptoms
- signs of acute renal failure
- vomit
- diarrhea
- blood loss
- shock
- altered mental status
- oliguria or polyuria
- signs of acute renal failure
- primary symptoms
- Physical exam
- signs of volume overload
- edema
- jugular venous distention
- signs of volume overload
- decreased breath sounds in pulmonary edema
Imaging
- Ultrasound
- indications
- if an obstruction needs to be ruled out (post-renal cause of AKI)
- best initial test
- findings
- can see hydronephrosis or stones
- indications
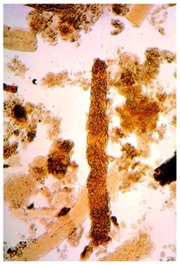
- Histology
- rarely obtained unless concerned about a concurrent glomerular process
- will show necrosis of tubular lining cells
Studies
- Labs
- serum potassium
- hyperkalemia during oliguric phase
- hypokalemia during polyuric phase
- anion gap metabolic acidosis
- ↑ BUN
- ↑ creatinine
- BUN:creatinine ratio < 15
- serum potassium
- Urinalysis with microscopy and sediment analysis
- Diagnostic criteria
- diagnosis of AKI
- ↑ serum creatinine of ≥ 0.3 mg/dL within 48 hours
- ↑ serum creatinine of 1.5 fold from baseline
- signs of acute tubular necrosis
- urine osmolality < 350-500 mOsm/kg
- muddy brown casts on urine sediment analysis
- fractional excretion of sodium > 2%
- diagnosis of AKI
- decreased BUN:creatinine ratio
Differential
- Prerenal azotemia
- BUN:creatinine ratio > 20
- Post-renal azotemia
- source of obstruction found on imaging
- e.g., stones or congenital abnormality
Treatment
- Conservative
- supportive care
- remove nephrotoxic agent
- intravenous hydration
- close electrolyte and fluid level monitoring
- indications
- for all with suspected acute tubular necrosis
- supportive care
- Medical
- renal replacement therapy (dialysis)
- indications
- signs of fluid overload
- indications
- renal replacement therapy (dialysis)
- toxic electrolyte levels
Complications
- Electrolyte abnormalities
- hypokalemia
- hyperkalemia
- Volume overload