Snapshot
- A 40-year-old man presents to his primary care physician with bilateral upper extremity weakness and sensory changes. He describes the sensory changes as “numb to pain and heat.” Approximately 8 months ago, he had a multiple sclerosis exacerbation that required hospitalization with intravenous methylprednisolone for 5 days. On physical exam, there is sensory loss to pain and temperature in a “cape-like” distribution of the upper extremity, as well as 4/5 strength. The patient is scheduled for an MRI of the spine. (Post-inflammatory syringomyelia)
Introduction
- Dermatomal maps reflect the sensory distribution for a specific level
- therefore, one can determine at which level (e.g., brainstem and spinal cord) the lesion is located
- recall that the primary sensory modalities tested on physical exam includes
- light touch
- pain
- temperature
- vibration
- proprioception
- recall that the primary sensory modalities tested on physical exam includes
- therefore, one can determine at which level (e.g., brainstem and spinal cord) the lesion is located
- The dorsal root ganglia contain cell bodies of spinal nerve sensory neurons
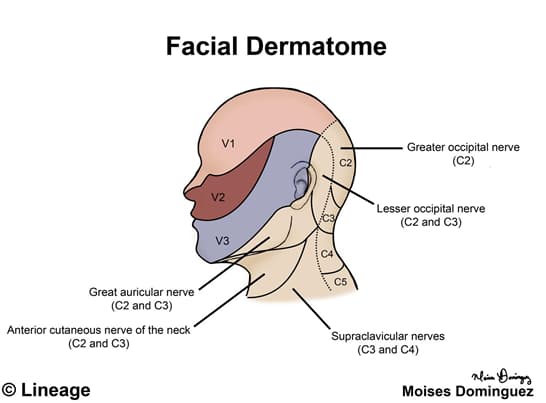
Head and Neck
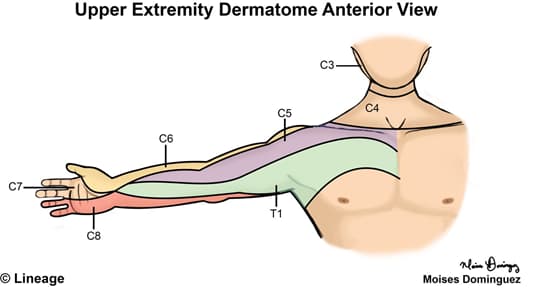
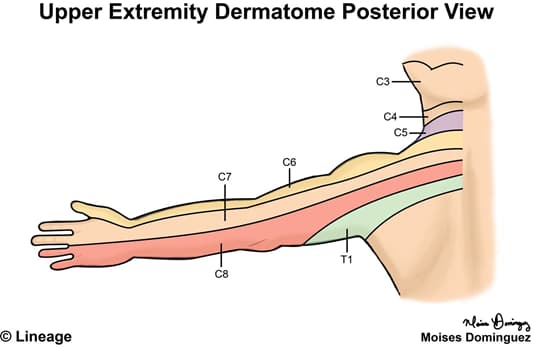
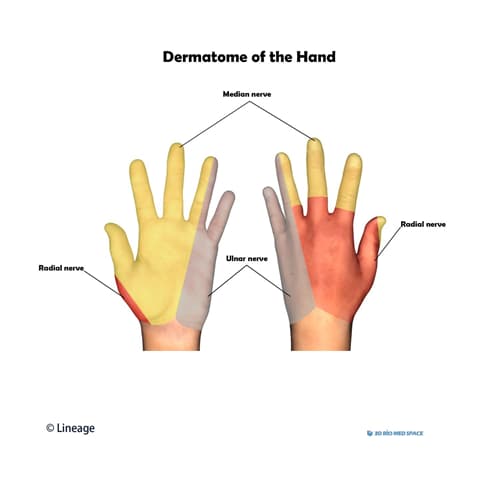
Hand
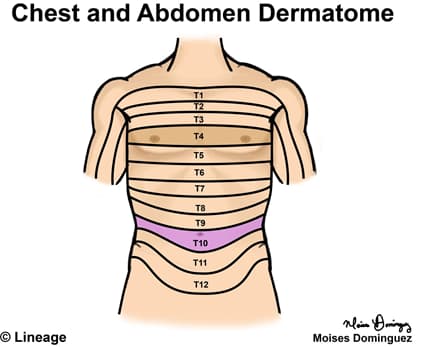
Chest and Abdomen
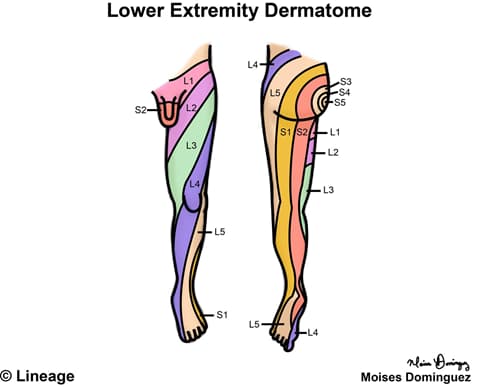
Lower Extremity