

Introduction
- An increase in serum calcium level
- Mechanisms and pathophysiology
- dietary causes
- calcium ingestion (milk-alkali syndrome)
- hypervitaminosis D
- hypervitaminosis A
- pharmacologic causes
- thiazides
- causes increased distal tubule reabsorption of calcium
- used to treat hypercalciuria
- thiazides
- malignancy-associated causes
- Paget’s disease
- typically does not result in hypercalcemia
- can be come hypercalcemic if patient is immobilized
- squamous cell cancer of the lung
- ectopic production of PTH (PTH related peptide – PTHrP)
- Paget’s disease
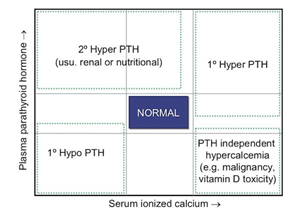
- hyperparathyroid
- genetic causes
- familial hypocalciuric hypercalcemia
- defect in calcium sensor of parathyroid gland
- there is a loss of negative feedback on PTH by hypercalcemia
- PTH levels are normal to high despite high serum calcium levels
- urine excretion of calcium is low
- key feature distinguishing primary hyperparathyroidism from FHH
- defect in calcium sensor of parathyroid gland
- familial hypocalciuric hypercalcemia
- dietary causes
- Zollinger-Ellison syndrome
Presentation
- Symptoms
- CNS
- confusion
- stupor
- weakness
- gastrointestinal
- constipation
- anorexia
- nausea
- vomiting
- kidney
- polyuria
- kidney stones
- polydipsia
- CNS
- Physical exam
- weakness
- decreased/absent reflexes
- EKG
- shortened QTc interval
Treatment
- Conservative
- hydration
- saline diuresis
- hydration
- Pharmacologic
- loop diuretics
- bisphosphonates
- mithramycin
- calcitonin
- galium nitrate
- Other
- dialysis