

Introduction
- Functional ovarian cysts
- ovarian follicular cysts
- corpus luteal cysts
- theca lutein cysts
- Other cysts
- dermoid cyst/teratoma
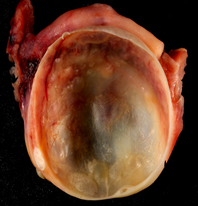
- endometriomas/chocolate cysts
- Evaluation
- ultrasound, CT or MRI
- Complications
- rupture or hemorrhage can cause peritonitis
- ovarian torsion
- often presents with nausea/vomiting and sharp, sudden lower abdominal pain
- caused by twisting of the infundibulopelvic ligament
Follicular Cyst
- Most common ovarian mass in women of reproductive age
- Non-neoplastic expansion of an unruptured graafian follicle
- Associated with hyperestrogenism and endometrial hyperplasia
- Evaluation with ultrasound
- thin walled
- unilocular
- Treatment
- large (>5cm) or symptomatic may undergo surgical resection
- small asytompatic cysts managed conservatively
Corpus Luteal Cyst
- Failure of corpus luteum to regress after ovum release
- Most common pelvic mass within 1st trimester of pregnancy
- Can result in complicating hemorrhage or rupture
- Evaluation with ultrasound
- diffuse thick wall
- peripheral vascularity/ “ring of fire”
Theca-Lutein Cyst
- Excessive circulating gonadotropins (beta-hcG) causes hyperplasia of theca interna cells
- Often bilateral and multicystic
- Associations with gonadotropin stimulation
- multifetal pregnancy
- PCOS
- clomiphene intake
- ovulation induction
- gestational trophoblastic disease
Dermoid cyst/ Teratoma
- Also known as mature cystic ovarian teratoma
- Most common ovarian neoplasm
- Contain elements from multiple germ layers (e.g. hair, skin or teeth)
- Slow growing and rarely cancerous
- Variant
- struma ovarii tumor: contains thyroid elements
Endometrioma/ “Chocolate Cyst”