

Snapshot
- A 25-year-old pregnant woman presents with fatigue and abdominal pain in the emergency room. She reports feeling unwell for the past few days. Every morning, she notices that her urine is tea-colored, which slowly resolves throughout the day. She has a low-grade fever. On physical exam, her skin is jaundiced, her liver edge is palpable, and she has abdominal tenderness to palpation. Her physicians are suspicious of Budd-Chiari syndrome.
Introduction
- Clonal stem cell defect from mutation in hematopoietic stem cell
- Pathogenesis
- mutation in PIGA gene
- defect in glycosylphosphatidylinositol (GPI) anchors CD55 (decay-accelerating factor) and CD59 on RBC membrane
- these protect RBC from complement
- “PNH Thrombosis”
- Pancytopenia
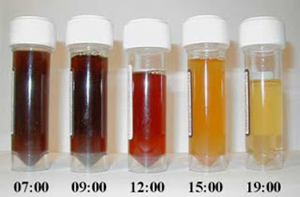
- with Nocturnal build up of dark urine
- Coombs negative Hemolytic anemia (complement-mediated)
- venous Thrombosis
- Acute hemolysis often triggered by stress, infection, surgery, and other inflammatory states
- May cause
- aplastic anemia
- myelodysplasia
- acute leukemia
Presentation
- Symptoms/physical exam
- episodic dark urine with first urine of the day
- caused by hemoglobin
- hemolytic anemia: pallor, fatigue, tachycardia, jaundice, and gross hematuria
- thrombocytopenia: mucosal bleeding, petechiae,and ecchymoses
- leukemia: infections
- thrombosis
- episodic dark urine with first urine of the day
- renal impairment
Evaluation
- Flow cytometry – most accurate test
- CD55/59-negative RBCs
- Labs
- anemia
- thrombocytopenia
- leukopenia
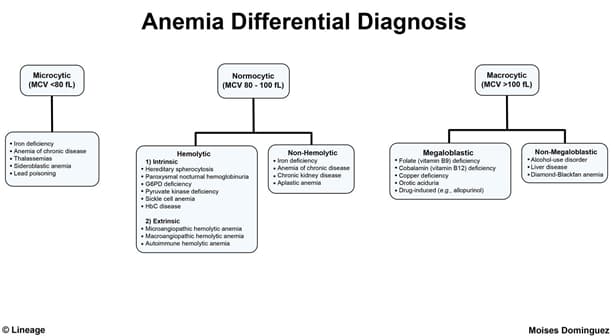
Differential Diagnosis
Treatment
- Eculizumab
- inactivates C5 in complement pathway
- decreases red cell destruction
- complement inhibitor
- must vaccinate all against Neisseria due to increased risk
- Allogeneic bone marrow transplant
- Supportive therapy
- folic acid
- transfusions as needed
Prognosis, Prevention, and Complications
- Prognosis
- improved with use of eculizumab
- Complications
- renal insufficiency
- thromboembolism
- 5% develop myelodysplasia
- 2.5% develop acute leukemias