

Snapshot
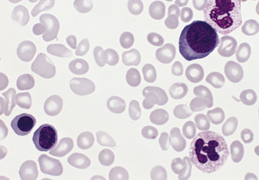
- A 59-year-old woman presents to her primary care physician with overwhelming fatigue, headaches, and some blurry vision. She is worried that old age is finally catching up. While she is happy about losing 10 lbs over the past month, she is also confused since she has not changed her diet or exercise routine. On further questioning, she reveals that she is extremely itchy after a hot bath or shower. She is otherwise healthy. A blood smear shows RBC precursors.
Introduction
- Myeloproliferative neoplasm characterized by increased production of RBCs
- leads to highly viscous blood
- Epidemiology
- presentation in those aged 60-70
- Pathogenesis
- mutations in JAK2 (Janus kinase)
- V617F mutation
- constitutively active Janus kinase → unregulated myeloproliferation
- erythrocytosis → ↑ blood viscosity
- leukocytosis
- thrombocytosis
- mutations in JAK2 (Janus kinase)
- Associated conditions
- risk of progression to myelofibrosis or leukemia
- Prognosis
- 1.6x higher mortality than general population
Presentation
- Symptoms
- headaches
- visual disturbance
- bleeding
- caused by engorged vessels
- constitutional symptoms
- fatigue
- night sweats
- weight loss
- fever
- malaise
- pruritus
- caused by histamine release from increased basophils
- often triggered by hot shower or bath
- Physical exam
- erythromelalgia (rare but classic)
- caused by thrombosis
- characterized by painful burning sensation with increased temperatures in digits and episodic blood clots in extremities
- hepatosplenomegaly
- bruising
- ischemic digits
- erythromelalgia (rare but classic)
- large retinal veins on funduscopy
Evaluation
- Labs
- complete blood count with smear will show
- ↑ hemoglobin > 16 g/dL (females) or > 16.5 g/dL (males)
- ↑ hct > 48% (F) or > 49% (M)
- JAK2 mutation in peripheral blood
- ↓ serum EPO
- ↑ RBC despite low EPO
- if EPO is high, consider ectopic EPO production (e.g., in renal cell carcinoma)
- ↓ MCV
- SaO2 normal
- complete blood count with smear will show
- Bone marrow biopsy
- shows hypercellularity and prominent proliferation of all cell lines
- commonly see precursor cells
- used to confirm diagnosis
- shows hypercellularity and prominent proliferation of all cell lines
- used as a baseline for assessing disease progression
Differential Diagnosis
- Secondary polycythemia
- Tumor-driven polycythemia
- Other myeloproliferative neoplasm
Treatment
- Reduce risk of thrombosis
- low-dose aspirin
- phlebotomy
- indicated for a hematocrit < 45%
- Myelosuppression
- hydroxyurea
- Gout prophylaxis
- allopurinol
Complications