

Snapshot
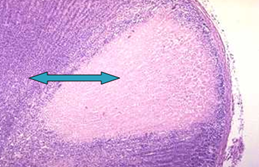
- A 68-year-old man presents to the emergency room with a 2-day history of abdominal pain, nausea, and vomiting. He denies any urinary frequency or urgency and denies any recent changes in his diet. His temperature is 100.4°F (38°C) and pulse is 104/min. He has a past medical history significant for type II diabetes mellitus and coronary artery disease. He has had two stents in the past three years. On physical exam, there is bilateral flank tenderness upon palpation. A non-contrast computerized tomography (CT) scan without contrast is negative for urolithiasis. A CT scan with contrast reveals a wedge shaped perfusion defect in both kidneys.
Introduction
- Clinical definition
- complete occlusion of main renal artery or segmental branch
- Epidemiology
- incidence
- very rare
- 0.7-1.4% found on autopsies
- risk factors
- cardiovascular disease
- incidence
- Etiology
- cardioemboli
- cardiomyopathy
- endocarditis
- artificial valves thrombi
- renal artery injury and thrombosis
- Marfan syndrome
- trauma
- polyarteritis nodosa
- other vasculitidies
- hypercoagulable states
- hereditary thrombophilia
- antiphospholipid syndrome
- cardioemboli
- Pathogenesis
- complete occlusion of main renal artery or segmental branch artery
- Associated conditions
- atrial fibrillation
- Prognosis
- 11-12% mortality in first month after diagnosis
- renal infarction occurs in patient populations with significant morbidity and mortality, such as atrial fibrillation
- 11-12% mortality in first month after diagnosis
- patients are at risk for future repeat renal infarctions
Presentation
- Symptoms
- acute onset abdominal or flank pain
- nausea
- vomiting
- Physical exam
- fever
- acute elevation in blood pressure
- may be mediated by renin release
- tenderness to palpation of abdomen or flank
- other signs of extrarenal embolization
- focal neurologic deficits
Imaging
- Spiral CT without contrast
- indications
- initial test for flank pain to evaluate for renal calculi
- indications
- CT with contrast
- indications
- if there are no calculi seen on initial imaging
- to evaluate for renal infarction
- indications
- 80% sensitivity
Studies
- Labs
- ↑ creatinine
- but it can also be normal if embolus is unilateral
- ↑ lactate dehydrogenase (> 2-4x upper limit of normal)
- little or no ↑ in serum aminotransferases
- ↑ creatinine
- Urine studies
- hematuria
- proteinuria
- Electrodiagnostics
- electrocardiogram to evaluate for atrial fibrillation
- Diagnostic criteria
- in the correct clinical context, the combination of elevated lactate dehydrogenase and normal serum aminotransferase is strongly suggestive of renal infarction
- note, this combination is also seen in transplant rejection, late myocardial infarction, and hemolysis, but these are clinically distinct from renal infarction
Differential
- Renal atheroemboli
- incomplete occlusion of distal vessels
- will likely have eosinophilia, eosinophiluria, and hypocomplementemia
- Nephrolithiasis
- stones seen on imaging
- lactate dehydrogenase is normal
Treatment
- Medical
- anticoagulation
- indications
- atrial fibrillation
- hypercoagulable state
- delayed diagnosiss
- anticoagulation therapy is prophylactic to prevent future events
- drugs
- heparin followed by warfarin
- indications
- anticoagulation
- Percutaneous endovascular therapy
- thrombolysis and thrombectomy
- indications
- in patients who are diagnosed early
- indications
- thrombolysis and thrombectomy
- if diagnosed early, viable tissue may be saved with thrombolysis
Complications
- Repeat thromboembolic events
- Renal failure