

Snapshot
- A 50-year-old man with a history of diabetes mellitus presents to the emergency room for gross amounts of blood in his urine. He denies any pain with urination and has never had hematuria before. He has no family history of cancer and does not smoke. Physical exam is unremarkable. His urinalysis reveals hematuria, proteinuria, and necrotic tissue.
Introduction
- Clinical definition
- necrosis and sloughing of renal papillae
- Epidemiology
- demographics
- middle-aged adults
- uncommon in children, except in those with sickle cell disease or trait
- demographics
- Pathogenesis
- due to ischemia
- in sickle cell trait or disease
- sickling is promoted in the renal medulla
- due to low oxygen tension, low pH, and high osmolality (pulling water out of red blood cell and increasing concentration of hemoglobin S)
- increased blood viscosity leads to infarcts and causes papillary infarcts
- sickling is promoted in the renal medulla
- in analgesic use
- NSAIDs inhibit prostaglandin synthesis (remember that prostaglandins vasodilate)
- this predisposes patients to renal hypoperfusion and ischemia, especially in those with pre-existing renal disease or any other risk factors for renal papillary necrosis
- Prognosis
- prognostic variable
- negative
- concomitant diabetes
- negative
- prognostic variable
- older age
Presentation
- Symptoms
- primary symptoms
- fever and chills
- sudden onset flank or abdominal pain
- may be asymptomatic
- hematuria
- pyelonephritis
- primary symptoms
- Physical exam
- tenderness to palpation in the flank or abdomen
Imaging
- Radiographs
- indications
- if obstruction, such as kidney stones, is suspected
- not diagnostic
- recommend views
- kidneys, ureters, and bladder (KUB)
- findings
- hydronephrosis from obstruction
- may visualize kidney stones
- indications
- CT
- indications
- typically performed if patients present with hematuria, even if renal papillary necrosis is suspected, as hematuria can indicate malignancy in the bladder
- views
- CT of abdomen and pelvis
- findings
- hydronephrosis
- kidney stones
- ring shadows in medullae
- loss of papillae
- indications
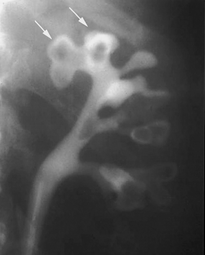
- Intravenous urography (IVU)
- indications
- if CT scan is inconclusive and suspicious for renal papillary necrosis remains high
- if there is no suspicion of obstruction but suspicion of renal papillary necrosis remains high
- findings
- indications
- ring shadow from desquamated papillae – “ring sign”
Studies
- Labs
- serum creatinine
- if there is a sudden rise in creatinine, consider renal papillary necrosis in patient with diabetes or chronic urinary obstruction
- serum creatinine
- Urinalysis
- hematuria
- pyuria
- proteinuria
Differential
- Nephrolithiasis
- kidney stone seen on imaging without evidence of renal papillary necrosis
- Tubulointerstitial nephritis
- often presents with rash, arthralgias, and eosinophilia in the urine
Treatment
- Medical
- supportive care with fluid resuscitation
- indications
- supportive care with fluid resuscitation
- for all patients
Complications
- Chronic pyelonephritis
- Sepsis